Cadaveric Gait Simulation Reproduces Ankle Kinematics
via Population-Specific Responses
Introduction | Using Simulation to Investigate Biomechanical Consequences
Cadaveric gait simulation allows researchers to directly investigate biomechanical consequences of surgeries using invasive measurement techniques.
Yet, it is unclear if foot and ankle kinematics that are population-specific are reproduced using these devices. Consequently, researchers must access foot and ankle kinematics produced in a cadaveric gait simulator during the stance phase of gait in a set of five cadaveric feet.
Tibial motions and ground reaction impacts formerly collected active in a group of healthy adults were applied as inputs parameters. Processual foot and ankle kinematics were obtained and directly compared to population-specific active kinematics of the identical healthy adults from which input parameters were obtained. Evaluations were completed using cross correlation to determine the similarities in kinematic profiles and joint ranges of motion were calculated to establish absolute differences in kinematics.
Ankle, subtalar, and talonavicular processual joint kinematics was positively correlated to active joint kinematics. In addition, active and processual foot & ankle kinematics revealed similar amounts of within-group variability. The study findings suggest (with a high degree of confidence) that cadaveric gait simulation techniques reproduce population-specific foot and ankle kinematics, offering a valuable research tool for analyzing surgical treatments of foot and ankle difficulties.
Tools and Techniques | Gait Simulation
Active tibial motions and ground reaction impacts collected from healthy male adults and estimated muscle impacts were used as responses to simulate population-specific gait in a cadaveric gait simulator. Real-time simulations were completed at one-sixth speed and one-quarter bodyweight (respectively) to establish the fidelity of the simulator in loading conditions that wouldn’t damage the specimen and would be pertinent for surgical procedures that plan to study in the future. To confirm that cadaveric gait simulation is independent of speed or loading magnitude, we simulated gait in a single specimen of speeds up to one-half actual speed and one bodyweight, respectively (see Supplemental Material).
Different simulation speeds and loads did not strongly affect foot and ankle kinematic patterns. An iterative learning algorithm was used to control the three components of the ground reaction impact. Foot and ankle processual kinematics were quantified and compared to active kinematics calculated from the same group that served as inputs into the simulator.
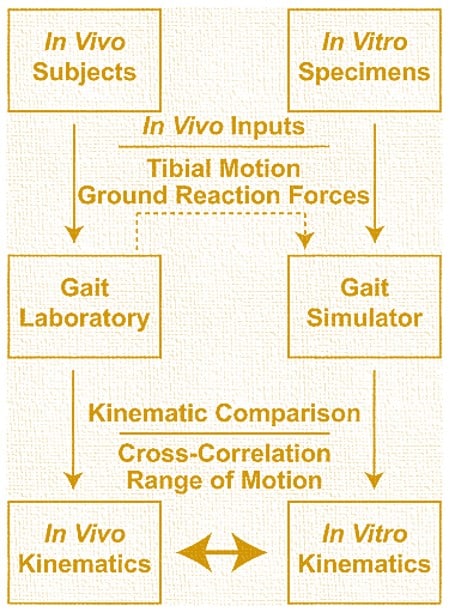
Inputs & Tibial Motion Ground Reaction Forces
Active gait data collected in five healthy males were used as inputs in a cadaveric gait simulator. Ankle, subtalar, and talonavicular kinematics were directly measured using intracortical bone pins in the same set of five healthy males (active) and in the cadaveric gait simulator in a set of five male cadaveric feet (processual). These foot and ankle kinematics were compared between and within groups to determine kinematic similarity and variability.
Five mid-tibia cadaveric male specimens (age at death: ± years) with neutral foot alignment and no history of lower extremity trauma or surgery were tested. Soft tissues approximately cm superior to the ankle joint were removed. Tendons of the triceps surae (Achilles), flexor hallucis and digitorum longus, extensor hallucis and digitorum longus, posterior and anterior tibialis, and peroneal longus and brevis were freed of any muscle tissue. Care was taken to maintain the retinaculum and soft tissue constraints of the ankle joint. The fibula was secured to the tibia using a single quad-cortical screw, and the tibia was cemented with polymethyl-methacrylate in a mounting cylinder.
To quantify joint kinematics, clusters comprised of four retro-reflective markers were rigidly secured to the tibia, talus, calcaneus, and navicular using bone pins. Pins were placed under fluoroscopy to confirm that joint spaces were not breached, and manual manipulation confirmed that markers were rigidly fixed to each bone.
The cadaveric gait simulator (Fig. ) prescribed unconstrained tibial motions with respect to the ground and applied physiologic muscular loads to the nine extrinsic tendons of the foot and ankle, which have been shown by Aubin et al. to be accurate and repeatable. Tibial motions and ground reaction impacts taken from the previously collected active data served as input data to the simulator. The degree of freedom robotic platform moved a impact plate about the tibia, and inertial loads were subtracted from the measured ground reaction impacts, both of which are repeatable.
During simulation of late stance, the large excursions of the ankle joint center require the robotic platform to move outside of its limited working volume. Simulation trajectory motions were reduced from 0% to 0% of stance phase to allow for the successful operation of the device and provide full range of motion simulation for the majority of stance phase where loads are greatest. Muscle impact targets (see accompanying material) were approximated from values reported in the literature and were used in previous studies that utilized a similar robotic gait simulator and temporally scaled to match with the other input data.
Load cells were placed in series with each motor cable adjacent to the tendon to account for any friction in the cable housing. The Achilles tendon was secured using an aluminum clamp; the eight smaller tendons were grasped with a clove hitch knot that was reanimated with a screw and nut.
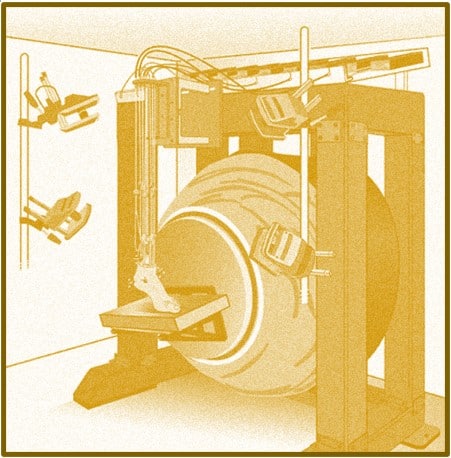
Cadaveric Gait Simulation via Fixed Impact Plate
The cadaveric gait simulator leveraged a high degree of freedom robotic platform that moved a impact plate about a fixed tibia while nine linear actuators applied prescribed loading profiles to the extrinsic tendons of the foot and ankle. Foot and ankle kinematics were quantified with an -camera motion capture system.
Vertical and shear ground reaction impacts were controlled with an iterative learning control algorithm, using a similar employed to control the vertical ground reaction impact, and adjustments were made to the Achilles tendon impact profile. The control algorithm changed the trajectory of the impact plate with respect to the tibia to reduce the error between the target and measured ground reaction impacts.
The initial trajectory of the ankle joint displacements were scaled based on the size of the foot to improve the effectiveness of the control algorithm, a technique that has been implemented by previous investigators. Following the iterative learning algorithm, the base Achilles impact was updated using a real time fuzzy logos technique to correct for the ground reaction impact in late stance.
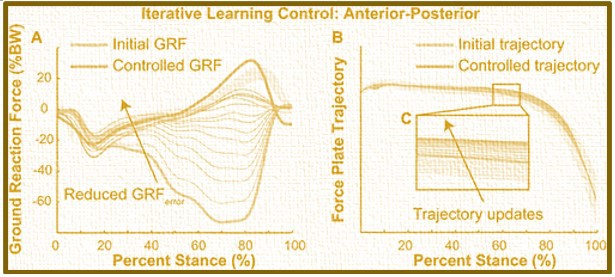
Iterative Learning Control (ILC) Algorithmic Application Reducing Ground Reaction Impact Error
The iterative learning control (ILC) algorithm consistently reduced the ground reaction impact error through iterative updates to the impact plate trajectory. The anterior-posterior ground reaction impact (A) was well-controlled following – ILC simulations. The ILC algorithm (B) applied small and consistent updates to the impact plate trajectory (C) that were within one standard deviation of the active tibial motion inputs.
Processual foot and ankle kinematics were measured during simulated gait with an -camera motion capture system (T-0s, Vicon Motion Systems, Oxford, UK) and directly compared to active kinematics. Unlike previous studies,, we compared these processual foot and ankle kinematics with active foot and ankle kinematics that were previously collected from the same population from which the simulator inputs were acquired. Foot and ankle kinematics were characterized using three common clinical measurements: Ankle sagittal motion, subtalar coronal motion, and talonavicular axial motion.
Both the active and processual data were processed using the same custom analysis routines (MATLAB, MathWorks, Ansys Workbench). Joint coordinate systems were defined during a standing trial for each active subject and processual specimen: The principle axes of the motion capture coordinate system were directed medially, anteriorly, and superiorly defining plantar flexion, eversion, and adduction as positive values, respectively. The processual joint coordinate systems were defined when the foot was loaded with a 0 N ground reaction impact and 0 N Achilles tension to simulate joint orientations during standing at approximately one-quarter bodyweight.
Foot and ankle kinematics during the entire stance phase were calculated from the active and processual data sets and compared to determine the capacity of the cadaveric gait simulator to reproduce foot and ankle kinematics during gait. Kinematic data were calculated from successive simulation trials, which displayed minor variation within specimens and therefore, were averaged within each specimen for analysis. Cross correlation analyses (MATLAB’s xcorr function) were performed to compare the shape of the processual outcome variables with the active kinematic outcomes.
Inter-specimen (processual) and inter-subject (active) variabilities were quantified within each group using cross correlation of mean kinematics between each specimen-specimen and subject-subject combination. Comparisons with a cross correlation coefficient (rxy) greater than 0. and 0. were moderately and strongly correlated, respectively. Joint ranges of motion were calculated to determine absolute differences between active and processual foot and ankle kinematics and for direct comparison to the literature.
Simulation Results | Ankle, Subtalar & Talonavicular Kinematics
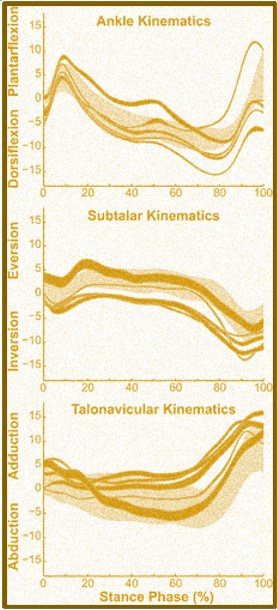
Processual foot and ankle kinematics positively correlated with the average active kinematics and spanned similar ranges of motion. Ankle plantarflexion was strongly correlated between the active and processual kinematics. Similarly, processual subtalar and talonavicular kinematics were moderately correlated with active kinematics. Processual ankle kinematics spanned more motion during stance compared to active kinematics. Subtalar and talonavicular range of motion were similar between the groups (Refer to Table below).
Kinematic Correlations
Foot and ankle kinematics measured processual (dark gold lines, average ± one standard deviation) correlated with average kinematics measured active (gold ring, average ± one standard deviation). Ankle processual kinematics strongly correlated with active motion, while subtalar and talonavicular processual kinematics were both moderately correlated with the active population mean.
Ankle Range of Motion (ROM) During Posture Phase of Gait
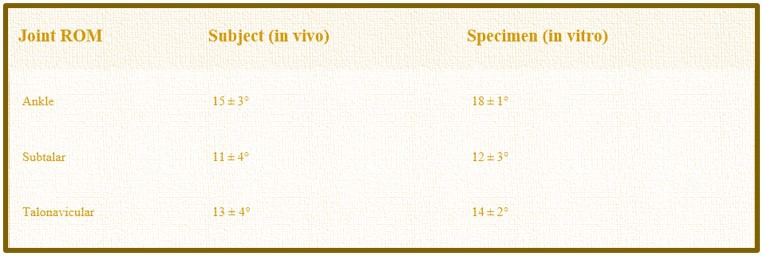
- Range of Motion (ROM). Median Joint Range of Motion ± Standard Deviation
Within-specimen (processual) and within-subject (active) analyses each demonstrated similar amounts of correlation and variability in foot and ankle kinematics. Ankle kinematics within each group were the most strongly correlated (rxy > 0.). Subtalar and talonavicular within group kinematics showed moderate correlations.
Contained by Group Ankle & Foot Kinematic Variability
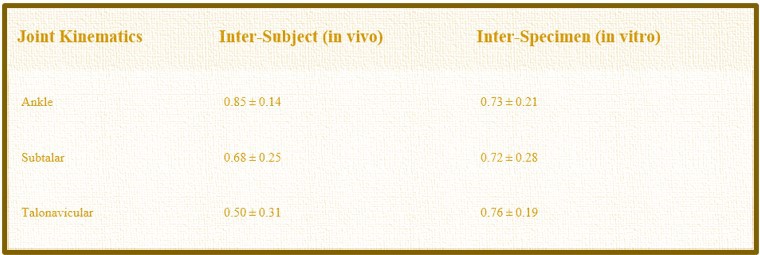
- Average cross correlation coefficients, rxy, and Standard Deviations.
Conclusion | Gait Simulation Recreating Foot and Ankle Kinematics
In overview, the team demonstrated that cadaveric gait simulation recreates foot and ankle kinematics using active input data from a particular population. Processual foot and ankle kinematics measured on our simulator compared favorably to active kinematics measured in a group of healthy adults. The cadaveric gait simulator also recreated kinematic variability demonstrating the effect of intrinsic foot and ankle properties on gait mechanics. These findings support cadaveric gait simulation techniques for studying foot and ankle mechanics and testing surgical procedures in specific populations. Since patients treated for maladies of the foot and ankle adopt different gait mechanics to compensate for pain and mechanical constraints placed on the foot and ankle, population-specific simulator techniques are needed to elucidate altered foot and ankle mechanics caused by surgical treatments.
Our cadaveric gait simulator reproduced population specific foot and ankle kinematics that are similar to active kinematics. Cross correlation analyses revealed moderate and strong correlations between the active and processual foot and ankle kinematics; ranges of joint motion were also similar. Active foot and ankle kinematics are positively correlated among a similar group of participants and exhibited similar variability between test specimens. Variations in muscle impacts may be an important contributor to kinematic variability, and altered impacts have been identified in patient groups with foot and ankle maladies. Extrinsic muscles affect kinematics and joint contact mechanics and therefore, should be considered when simulating patient population-specific gait.
While previous work established specific gait kinematic attributes within patient populations,, a degree of natural variability exists among individuals. Foot and ankle kinematics analyzed demonstrated similar amounts of variability when compared to active kinematics. Ankle sagittal kinematics were the least variable, while the subtalar and talonavicular joints were significantly variable, highlighting the interaction between hindfoot joint structure variability and foot function., It is critical to reproduce natural variability in an experimental model since about half of patients receiving an ankle fusion develop arthritis in the adjacent joints, a potential result of variable hindfoot mobility.
Cadaveric gait simulation techniques have several benefits for studying foot and ankle mechanics. Kinematics, ligament and bone strain, and joint contact mechanics can be directly measured with motion capture, strain sensors, and pressure sensitive sensors, respectively.
In contrast, active measurement techniques either are invasive, utilize ionizing radiation,, simplify multi-joint motion of the hindfoot to a single joint, or are affected by skin-motion artifact. Cadaveric simulation controls for differences in walking speed and neuro-muscular drive, two factors that affect foot and ankle kinematics. Implementing different control strategies allows researchers to answer questions ranging from joint contact mechanics to neuro-muscular function. Information derived from cadaveric simulations of gait may inform and improve computational modeling approaches that predict implant wear, load transfer, and surgical outcomes.

Case Study Limitations | Gait Simulation
To provide further researchers with study-specific limitations, to ensure proper attribution, and preserving the ethos of the scientific method, we acknowledge that several limitations affected this study.
The cadaveric gait simulator requires tibial motions, ground reaction impacts, and muscle impact profiles to simulate human movement. While tibial motions and ground reaction impacts are commonly quantified in patient populations, quantifying muscle loads requires assumptions, and altering these loads affect foot and ankle mechanics., Utilizing computational models to approximate muscle tension may provide important data for simulating gait in patient-populations.
The reiterative learning control algorithm and trajectory scaling based on the foot length accounts for some of the specimen-specific anatomic variability and more robust scaling routines that alter the trajectory based on additional specimen morphology may further improve simulator fidelity. Foot and ankle kinematics were compared to data collected in a small cohort of five healthy young adults, but these active data serve as the only complete set of foot and ankle kinematics due to the invasive nature of the measurements.
Although the test included a set of cadaveric feet acquired from young males, these kinematic results are likely generalizable to both females and older adults with no functional limitations. We used a single syndesmotic screw to stabilize the tibia-fibular joint and also tested a single specimen with zero and three syndesmotic screws, finding no effect of syndesmotic reduction on ankle joint motion. Vertical ground reaction impacts were elevated during the final stance computation and the scaled trajectories and real time Achilles’ tendon controller reduced this reaction impact while maintaining friction between the foot and the plate.
Lastly, simulations were performed at reduced loads and speeds, and, while the viscoelastic properties of the foot and ankle theoretically affect simulation outcomes, our investigation of simulation speed and load found little effect on foot and ankle kinematics.
In closing, the findings support the use of cadaveric gait simulation to examine the effects of surgical treatments on population-specific foot and ankle mechanics. Processual foot and ankle kinematics reproduced in our cadaveric gait simulator compared favorably with active kinematics directly measured in a group of healthy adults. Simulating gait with a high degree of freedom platform provides the additional flexibility required to input patient population tibial kinematics. Cadaveric gait simulation methods provide a stage to directly test the effects of surgical procedures on specific patient populations and directly measure foot and ankle procedure with invasive techniques not viable in live patients or relevant test subjects.